The patient is a 60-year-old male who has undergone two surgeries due to chest wall infection. In 2015, the patient underwent a decortication procedure for empyema. However, his incision did not heal properly after the surgery and persistently oozed pus, causing him great pain. In 2017, to treat the recurring chest wall infection, he underwent a second operation. Regrettably, the incision once again failed to heal and continued to ooze pus.

Previous Case
Chest Wall Tumor Resection and Chest Wal...

Next Case
A 16-year-old Patient with Severe and Ra...
Medical History
Preoperative Examination
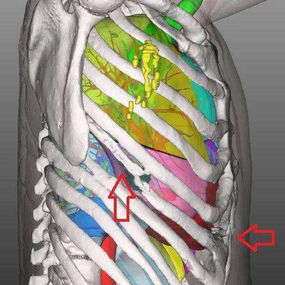
A 30-centimeter-long scar from previous surgeries is present on the right chest wall, with two areas of ulceration—one near the xiphoid process and the other along the anterior axillary line—both of which are oozing pus. A part of the right pleura thickens, and the sixth rib has deformed and fused with the seventh rib. Additionally, structural change is observed in the right costal arch. The patient was conclusively diagnosed with chest wall infection after chest wall surgery.
Surgical Overview
Explore the case of a 60-year-old male who required a third surgery following two unsuccessful attempts due to recurrent chest wall infection. Preoperative exam revealed two areas of ulceration, both are oozing pus. The surgery involved the resection of parts of the affected ribs, costal arch, and sternum, followed by lifting the right diaphragm to strengthen the chest wall at the defect and prevent abnormal breathing postoperatively.
Related Photos




Surgical Analysis
Due to this patient's long medical history, although the visible lesion appears localized, the underlying lesions are considerably larger in scope. The infected regions involve the 5th, 6th, and 7th ribs, the intercostal muscles, the costal arch, and the lower part of the sternum. If these potential lesions are not completely removed, the incisions may initially heal but are likely to rupture and ooze pus again. Thus, the surgical approach involved not only excising the lesions but also extensively removing all necrotic tissue to ensure a successful outcome.
Significant removal of bone structure can result in chest wall defect. Large defect typically requires chest wall reconstruction. However, reconstruction involves the use of synthetic materials, which could potentially interfere with the healing of the surgical site. Therefore, reconstruction was not performed in this case. Chest wall defects, however, could lead to paradoxical breathing, which may even impair the patient’s respiratory function. To avoid this situation, the diaphragm was artificially lifted upwards to bring it as close as possible to the 4th rib, thereby strengthening the chest wall at the defect and preventing paradoxical breathing after the surgery.



